Case Study
A 4-year-old male is brought into your trauma room after a high speed motor vehicle collision. There were two fatalities in the same vehicle. He was in the rear, restrained appropriately in his car seat. Vital signs are:
Heart Rate – 190 beats/minute
Respirations – 36 breaths/minute
Blood Pressure – 72/48
Capillary Refill Time – 3 seconds
His skin is cool and pale. There is a gross deformity and bleeding open fracture to the right femur. He has a “seatbelt sign” as noted by patterned abrasions on his abdomen. He opens his eyes only to verbal command, localizes to painful stimuli, and moans. His estimated weight is 40lbs.
How should we approach this situation?
Heart Rate – 190 beats/minute
Respirations – 36 breaths/minute
Blood Pressure – 72/48
Capillary Refill Time – 3 seconds
His skin is cool and pale. There is a gross deformity and bleeding open fracture to the right femur. He has a “seatbelt sign” as noted by patterned abrasions on his abdomen. He opens his eyes only to verbal command, localizes to painful stimuli, and moans. His estimated weight is 40lbs.
How should we approach this situation?

As always, you will use the ABCDE (airway, breathing, circulation, disability, exposure/environment control) method of primary assessment for this patient
The focus of this module will be on “C” – circulation so start there as a focus for this case study
Look for and control external hemorrhage: active bleeding from right thigh is identified and controlled with direct pressure
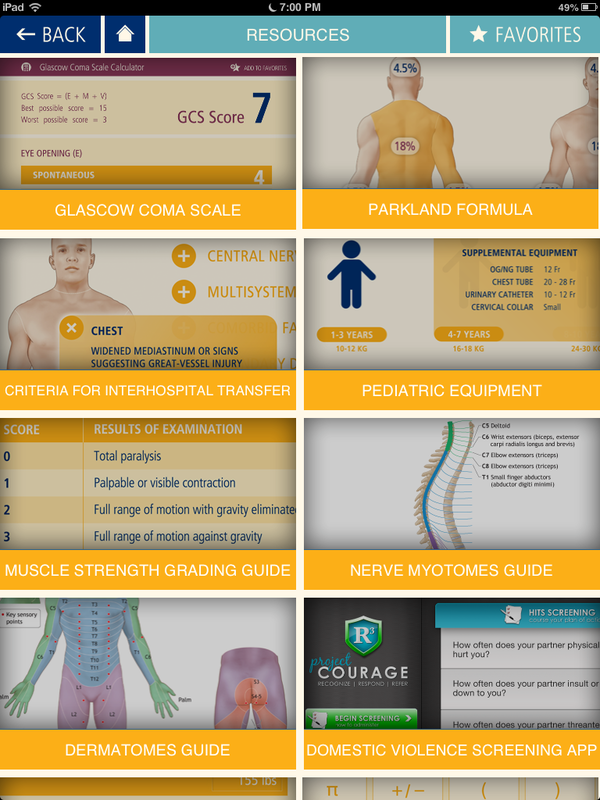
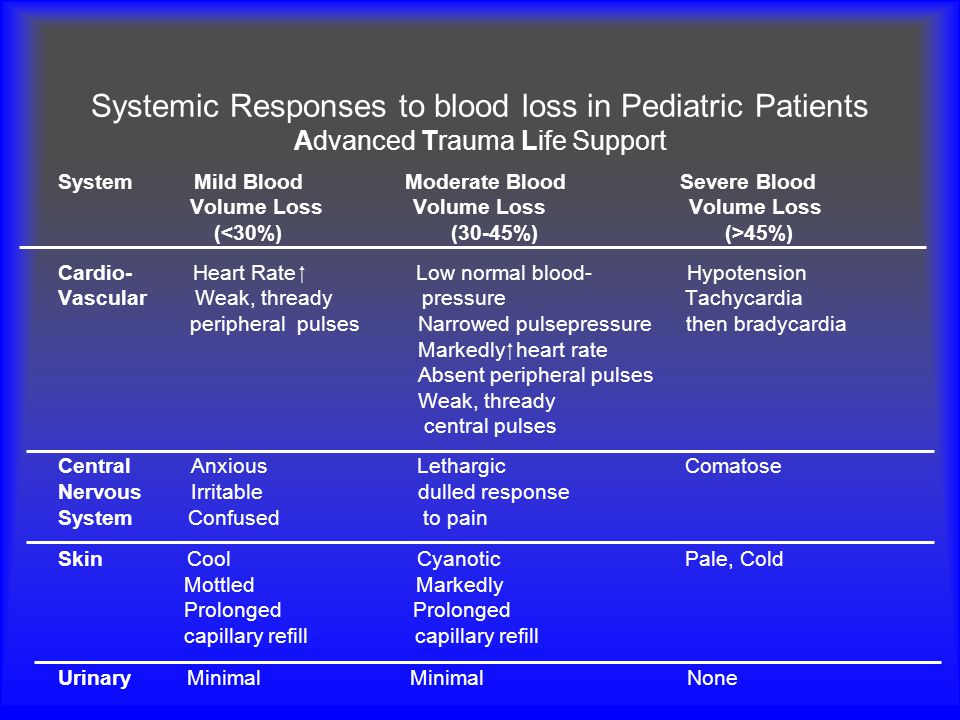
Evaluate level of consciousness (LOC) to help determine state of shock (see Pediatric GCS table)
Observe general appearance: patient is cold and pale
Observe body surfaces for injury. Abdomen has bruising and abrasions. The incidence of intra-abdominal injury is markedly higher if abdominal contusions identified
Evaluate peripheral and central pulses: Patient is tachycardic for age, heart tones audible, not muffled. Peripheral pulses are thread
***IT IS HERE YOU SHOULD INITIATE FLUID RESUSCITATION ***
Establish two IV lines (or IO) and collect blood samples. Consider IO after 2 unsuccessful peripheral IV attempts. See your module resource videos for tips on establishing access
Calculate warmed crystalloid amount
Frequent reassessment; determine if second crystalloid bolus is required and/or blood products
Complete frequent neurovascular checks of right leg, elevate, immobilize, consult orthopedic physician
In addition to improved assessment, a urinary output of 1 to 2 ml/kg/hr indicates a return to hemodynamic normality. A patient with minimal or no urinary output is experiencing moderate to severe blood loss
The focus of this module will be on “C” – circulation so start there as a focus for this case study
Look for and control external hemorrhage: active bleeding from right thigh is identified and controlled with direct pressure
Evaluate level of consciousness (LOC) to help determine state of shock (see Pediatric GCS table)
Observe general appearance: patient is cold and pale
Observe body surfaces for injury. Abdomen has bruising and abrasions. The incidence of intra-abdominal injury is markedly higher if abdominal contusions identified
Evaluate peripheral and central pulses: Patient is tachycardic for age, heart tones audible, not muffled. Peripheral pulses are thread
***IT IS HERE YOU SHOULD INITIATE FLUID RESUSCITATION ***
Establish two IV lines (or IO) and collect blood samples. Consider IO after 2 unsuccessful peripheral IV attempts. See your module resource videos for tips on establishing access
Calculate warmed crystalloid amount
Frequent reassessment; determine if second crystalloid bolus is required and/or blood products
Complete frequent neurovascular checks of right leg, elevate, immobilize, consult orthopedic physician
In addition to improved assessment, a urinary output of 1 to 2 ml/kg/hr indicates a return to hemodynamic normality. A patient with minimal or no urinary output is experiencing moderate to severe blood loss
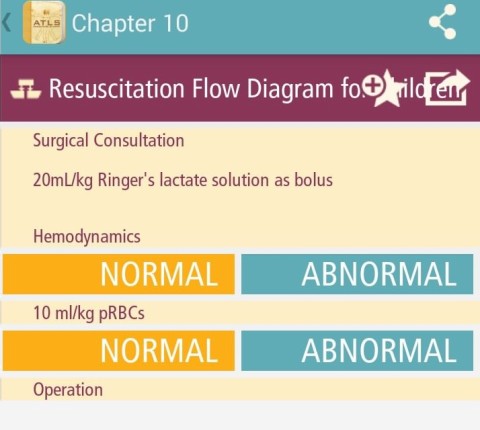
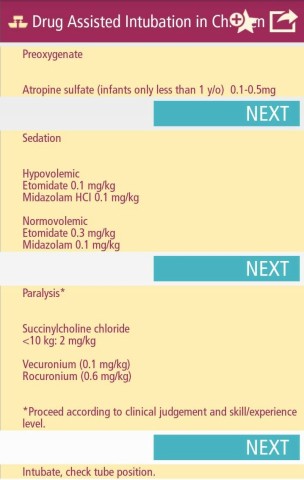
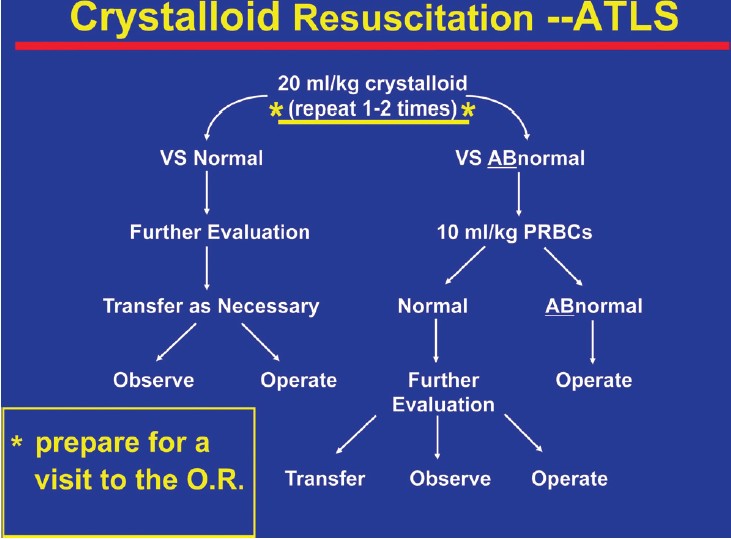
Tip: ATLS application for phone/tablet available with your textbook for the course. Notice the resuscitation flow diagram for children. Administer fluid boluses, administer blood products, if still abnormal response the child will require an operation. Also notice that certain medications such as sedation are calculated by whether or not child is hypovolemic
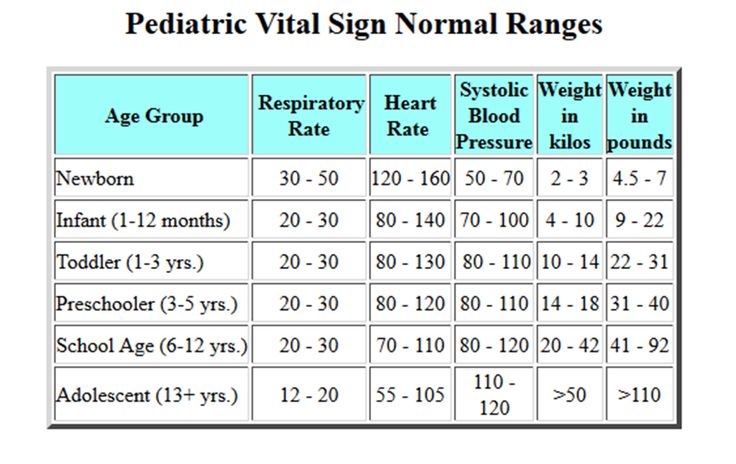
Normal Pediatric Vital Signs
It is extremely important to understand normal ranges for pediatric vital signs when determining need for resuscitation. See below for normal ranges by age. Also available on ATLS app.
QUICK CALCULATION FOR BLOOD LOSS
MILD BLOOD LOSS
(80-90 + 2 x age in years)
MODERATE BLOOD LOSS
(70-80 + 2 x age in years)
SEVERE BLOOD LOSS
(<70 + 2 x age in years)
QUICK CALCULATION FOR BLOOD LOSS
MILD BLOOD LOSS
(80-90 + 2 x age in years)
MODERATE BLOOD LOSS
(70-80 + 2 x age in years)
SEVERE BLOOD LOSS
(<70 + 2 x age in years)
Dosage Calculations

|

|

Calculations - You try!
The physician orders a Lactated Ringer's bolus for your patient. How many mL will you administer?
Two boluses of LR have been ineffective in resuscitation. How many mL of PRBCs will you administer?
When the patient arrived, did is blood pressure indicate mild, moderate or severe blood loss?
What do you anticipate as the plan for this patient?
What urinary output would indicate that resuscitation is effective?
Check your answers and then continue to your timed quiz on Module 2. If needed, use the HELP! option on the Home page for questions or troubleshooting before taking your Module 2 quiz.
Two boluses of LR have been ineffective in resuscitation. How many mL of PRBCs will you administer?
When the patient arrived, did is blood pressure indicate mild, moderate or severe blood loss?
What do you anticipate as the plan for this patient?
What urinary output would indicate that resuscitation is effective?
Check your answers and then continue to your timed quiz on Module 2. If needed, use the HELP! option on the Home page for questions or troubleshooting before taking your Module 2 quiz.
